What is a Varicocele?
A varicocele is caused by dilatation of the pampiniform plexus of spermatic veins (Figure 1). It is present in 15 to 20 % of post-pubertal males, 10-15% of unmarried military recruits, 35 % of infertile men who have never fathered a child and 81 % of men who were once fertile but are now infertile (secondary infertility). Left-sided varicoceles are 10 times more common than right-sided ones. They are commonly diagnosed clinically and on an ultrasound.
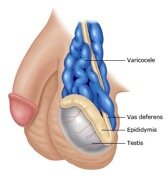
Figure 1. A varicocele is a collection of dilated and tortuous veins in the pampiniform plexus surrounding the spermatic cord. On physical examination, the spermatic cord has a “bag of worms” appearance that increases with standing or the valsalva manoeuvre.
The reason for the left-sided predominance may be explained anatomically. The left spermatic (gonadal) vein is one of the longest veins in the body, entering the left renal vein at a perpendicular angle. The intravascular pressure in the left renal vein is higher than on the right because it is compressed between the aorta and the superior mesenteric artery coming off the aorta above the renal vein, thereby producing a “nutcracker effect.” This phenomenon causes increased pressure in the left gonadal vein, which can dilate and cause incompetence of the valve leaflets, leading to retrograde flow of blood toward the testis in the erect position. The venous complex in the scrotum dilates and produces anything from minimal fullness on Valsalva manoeuvre to a large soft scrotal mass (“bag of worms”) that decompresses and disappears in the recumbent position.
Bilateral varicoceles occur in 33 %. Unilateral right varicoceles are very rare and may be associated with an underlying pathology causing inferior vena caval obstruction (renal cell carcinoma with IVC thrombus, right renal vein thrombosis with clot propagation down the IVC, etc).
Varicoceles are graded I, II, or III, according to size (Table 1).
| Grade | Size | Clinical description |
| 1 | Small | Palpable only with valsalva manoeuvre |
| 2 | Moderate | Nonvisible on inspection, but palpable upon standing |
| 3 | Large | Visible on gross inspection |
Table 1. Grading of varicocoeles
What are the symptoms?
Varicoceles may be asymptomatic (be without symptoms) or may cause any or all of the following:
- Dull, aching left scrotal pain, typically noticeable when standing and relieved by recumbency
- Feeling as though 1 testicle is heavier than the other
- Testicles that look different in size
- Testicular atrophy, believed to be secondary to loss of germ cell mass by induction of apoptosis (programmed cell death) initiated by the associated slightly increased scrotal temperature
- Compromised fertility
Although the presence of a varicocele can be associated with normal semen parameters and normal fertility, most men with varicocele and presumptive infertility have abnormal semen parameters, including low sperm concentration and abnormal sperm morphology. In a World Health Organization (WHO) study of over 9000 men who were partners in an infertile couple, a varicocele was much more common in men with abnormal semen (25.4 versus 11.7 % with normal semen). The causal relationship between varicocele and male infertility has been ascribed to increased testicular temperature, delayed removal of endogenously derived toxic materials and metabolites, hypoxia, and stasis (1).
What treatment options are available?
Surgical treatment involves ligating (tying or occluding) the gonadal vein so that retrograde (back flow) blood can no longer reach the plexus of veins in the scrotum. Treatment approaches include retroperitoneal, inguinal, sub-inguinal, microsurgical and laparoscopic (Figure 2). Treatment with gonadal vein embolization is an alternative performed by a radiologist (X-ray doctor), but there have been some reports of embolization coils migrating to other organs and with a higher failure rate (2).
Who should consider treatment?
Treatment is indicated for boys who demonstrate reduced growth of the left testis and in young men who develop testicular atrophy (loss of size). Catch-up growth of the atrophic testis is possible in some cases after surgery and the return of testicular size postoperatively directly correlates with normal fertility potential (3).
Treatment may be performed for patients who are very symptomatic from pain which is interfering with their daily activities and quality of life. Recent studies report an improvement in pain in 70-80% of cases after a microsurgical procedure (4).
Conservative treatment with a scrotal support and NSAIDs may suffice for an older man who has completed his family and who presents with minor scrotal discomfort as his only symptom.
Microsurgical Varicocelectomy
Microsurgical varicocelectomy has become the gold standard in adults because of low recurrence and postoperative hydrocele rates (5).
The goals of varicocele repair are to relieve pain in symptomatic cases and to improve semen parameters, testicular function, and pregnancy rates in couples with male factor infertility associated with varicocele. Studies have shown that varicocele repair can improve all three of these parameters in
60 to 80 % of men (6). In addition, varicocelectomy has been reported to improve sperm DNA integrity and stability (7;8). This in turn has been found to be associated with a higher pregnancy rate (9). In infertile men with low serum testosterone levels, microsurgical varicocelectomy has been shown to improve serum testosterone levels (10).
There are a number of different techniques available however it is important to use a technique that minimizes the risk of complications and recurrence.
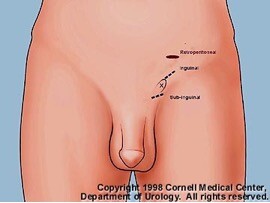
Figure 2. Retroperitoneal, inguinal, and subinguinal incisions for varicocele repairs. A dot is made to mark the external inguinal ring (X).
The advantages of the microsurgical sub-inguinal approach to varicocele repairs are reliable identification and preservation of the testicular artery or arteries, cremasteric artery or arteries, and lymphatic channels and reliable identification of all internal spermatic veins and gubernacular veins. Delivery of the testis assures direct visual access to all possible routes of venous return, including external spermatic, cremasteric, and gubernacular veins.
Postoperatively, venous return is via the vasal veins, which drain into the internal pudental system and usually have competent valves.
In the largest published study using the microsurgical technique pregnancy rate was 43 % after one year and 69% after 2 years compared to 16% in couples with men who declined surgery and had hormone treatment or used insemination. Moreover, the recurrence rate was only 1% and there were no reports hydrocele or testicular atrophy (11).

Figure 3. Under the operating microscope, the spermatic cord is examined. The internal and external spermatic fasciae are incised longitudinally and retracted with the straight clamps.

Figure 4. The artery is microscopically dissected free of all surrounding tissue, tiny veins and lymphatics. A 0-silk ligature is encircled for identification and preservation of artery.
The use of a microscope enables a surgeon to find and preserve the tiny artery that brings blood to the testes. Magnification also allows identification and preservation of the lymphatics, eliminating the risk of hydrocele (bag of water forming around the testis) after surgery.

Figure 5. Periarterial veins are lighted with 4-0 silk ligature. Hemoclips placed on the internal spermatic veins.
This technique is performed through a small incision and almost always as a day case procedure. Interventional radiologists can also fix varicocoeles by putting coils in the abnormal veins, through a small incision in the upper thigh, however this has a higher failure rate. Laparoscopy can also be used in men to repair varicoceles successfully. However, this is now very seldom performed as it is more invasive than the microsurgical method and risks injuring organs inside the abdomen.
Table 2. Techniques of Varicocelectomy
| Technique | ArteryPreserved | Hydrocele
(%) | Failure
(%) | Potential for Serious Morbidity |
| Retroperitoneal | NO | 7 | 15 -25 | NO |
| ConventionalInguinal | NO | 3 -30 | 5 – 15 | NO |
| Laparoscopic | YES | 12 | 5 – 15 | YES |
| MicroscopicInguinal | YES | O | 1 | NO |
The most common complications from varicocelectomy are hydrocele, varicocele recurrence, and testicular artery injury. Use of the operating microscope allows for reliable identification of spermatic cord lymphatics, internal spermatic veins and venous collaterals, and the testicular artery or arteries so that the incidence of these complications can be reduced significantly. Delivery of the testis through a small subinguinal incision provides direct visual access to all possible avenues of testicular drainage. Microsurgical varicocelectomy provides a safe and effective approach to varicocele repair with preservation of testicular function, improvements in semen quality, and improvements in pregnancy rates in a significant number of men.
Reference List
(1) Eisenberg ML, Lipshultz LI. Varicocele-induced infertility: Newer insights into its pathophysiology.
Indian J Urol 2011 Jan;27(1):58-64.
(2) Cassidy D, Jarvi K, Grober E, Lo K. Varicocele surgery or embolization: Which is better? Can Urol
Assoc J 2012 Aug;6(4):266-8.
(3) Li F, Chiba K, Yamaguchi K, Okada K, Matsushita K, Ando M, et al. Effect of varicocelectomy on testicular volume in children and adolescents: a meta-analysis. Urology 2012 Jun;79(6):1340-5.
(4) Kim SO, Chung HS, Park K. Modified microsurgical subinguinal varicocelectomy without testicular delivery. Andrologia 2011 Dec;43(6):405-8.
(5) Mirilas P, Mentessidou A. Microsurgical subinguinal varicocelectomy in children, adolescents, and adults: surgical anatomy and anatomically justified technique. J Androl 2012 May;33(3):338-49.
(6) Schauer I, Madersbacher S, Jost R, Hubner WA, Imhof M. The impact of varicocelectomy on sperm parameters: a meta-analysis. J Urol 2012 May;187(5):1540-7.
(7) Zini A, Azhar R, Baazeem A, Gabriel MS. Effect of microsurgical varicocelectomy on human sperm chromatin and DNA integrity: a prospective trial. Int J Androl 2011 Feb;34(1):14-9.
(8) Wang Y, Zhang W, Li D. [High ligation of varicocele improves sperm DNA integrity in patients with asthenospermia]. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2012 Dec;37(12):1228-32.
(9) Smit M, Romijn JC, Wildhagen MF, Veldhoven JL, Weber RF, Dohle GR. Decreased Sperm DNA Fragmentation After Surgical Varicocelectomy is Associated With Increased Pregnancy Rate. J Urol
2013 Jan;189(1 Suppl):S146-S150.
(10) Fisch H, Hyun G. Varicocele repair for low testosterone. Curr Opin Urol 2012 Nov;22(6):495-8.
(11) Goldstein M, Gilbert BR, Dicker AP, Dwosh J, Gnecco C. Microsurgical inguinal varicocelectomy with delivery of the testis: an artery and lymphatic sparing technique. J Urol 1992 Dec;148(6):1808-11.









