Renal and ureteric stones, Windsor and Berkshire
INTRODUCTION
Approximately 10 to 20 per cent of all kidney stones require surgical removal, which is determined based upon the presence of symptoms and the size and location of the stones. Larger stones and proximal ureteric stones are less likely to pass spontaneously.
Stone removal is also indicated for pain or obstruction or for an infected struvite stone.
Three minimally invasive surgical techniques that significantly reduce the morbidity of stone removal are currently available:
Rigid and flexible ureteroscopy with laser (URS)
Percutaneous nephrolithotomy (PCNL)
Shock wave lithotripsy (ESWL)
These techniques offer comparable success when compared with open surgery, and provide significant advantages in terms of patient morbidity and cost. In addition, improvements in urological equipment, X-RAY technology and interventional techniques provide many additional treatment options.
The choice of intervention for stones that are unlikely to pass spontaneously varies with the location and size of the stone. Studies suggest that either URS is an excellent option for managing ureteric calculi. ESWL is the treatment of choice for most small renal calculi, while PCNL is the preferred method of stone removal for larger (>1.5 cm) renal stones, including staghorn calculi.
Occasionally, a nephrostomy tube may need to be placed as an emergency temporizing measure, usually for patients who present with an obstructing stone and sepsis. Proper drainage of the infected urine is essential. Once the infection has cleared, the stone may be removed by one of the methods previously listed.
URETEROSCOPY AND HOLMIUM LASER
The development of the fibre optic ureteroscope technology has had a significant impact upon the management of ureteric and renal stones. Ureteroscopy is now the gold standard treatment of choice for middle and distal ureteric stones [8], but also can be used to safely and effectively manage proximal ureteric and intra-renal
calculi. In addition, ureteroscopy may be safely used for the management of ureteric and intra-renal calculi which have failed shock wave lithotripsy (ESWL) [9-11].
The Procedure
This is performed under a general anaesthetic either as a day case or with an overnight stay if required. You will usually be given an injectable antibiotic before the procedure, after checking for any allergies.
A telescope is inserted into the bladder through the water pipe (urethra). Under X-ray screening, a flexible guidewire is inserted into the affected ureter up to the kidney. A longer telescope (either rigid or flexible) is then inserted into the ureter and passed up to the kidney. The stone is disintegrated using a holmium laser and the fragments extracted with special retrieval devices. A ureteric stent is normally left in place, together with a bladder catheter after the procedure.
Rigid ureteroscopy
If the obstructing stone is small enough to be extracted intact, stone baskets or grasping forceps can be employed for stone removal. If, however, the stone is too large for intact extraction and requires fragmentation prior to removal, laser fragmentation is utilized to perform “intracorporeal lithotripsy.”
We routinely employ a state of the art 6 French semi-rigid ureteroscope combined with intracorporeal laser lithotripsy to manage stones of all sizes in the ureter.
Flexible ureteroscopy
Further innovations in fibre optic technologies have propelled the development of flexible ureteroscopes which can bend to greater than 270 degrees. This has enabled routine diagnostic and therapeutic procedures to be performed within the ureter and kidney. As an example, patients who present with haematuria and a filling defect of the upper pole collecting system can undergo direct visualization of the upper urinary tract. A therapeutic procedure, such as extraction of symptomatic lower pole renal calculi, can also now be performed with these devices with minimal trauma and side effects.
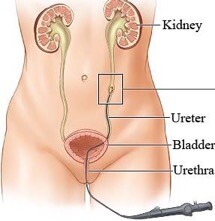
Figure 2. Flexible ureteroscopy being performed on left sided ureteric stone
Side Effects associated with Ureteroscopy and holmium laser
Common (greater than 1 in 10)
Mild burning or bleeding on passing urine for short period after operation
Temporary insertion of a bladder catheter
Insertion of a stent with a further procedure to remove it (usually after 2 weeks) The stent may cause pain, frequency and bleeding in the urine (10-25%)
Occasional (between 1 in 10 and 1 in 50)
Inability to retrieve the stone due to the ureter being physiologically tight (5-10%) during the first procedure
Kidney damage or infection needing further treatment
Failure to clear the stones fully especially if stones > 1cm in size and very hard in consistency
Recurrence of stones
Rare (less than 1 in 50)
Damage to the ureter with need for open operation or tube placed into kidney directly from back to allow any leak to heal
Very rarely, scarring or stricture of the ureter requiring further procedures
PERCUTANEOUS NEPHROLITHOTOMY (PCNL)
PCNL and open surgery are equally effective for the management of large renal stones [1]. An important difference is that PCNL shortens the hospitalization time by 60 per cent and allows the patient to return to work in approximately one week as compared to greater than three weeks after open renal surgery. Although this less invasive technique required special equipment and expertise, it is less expensive for the local health care economy [2].
Indications
Percutaneous stone removal procedures are currently reserved for patients with the following clinical characteristics [3-5]:
Large (>1.5 cm in diameter) or complex calculi (filling the majority of the intrarenal collecting system, such as staghorn calculi)
Cystine stones (relatively resistant to shock wave lithotripsy)
Anatomic abnormalities, including horseshoe kidneys or ureteropelvic junction obstruction
Stones within calyceal diverticula
The Procedure
Technical advances have resulted in considerable refinement of the percutaneous approach to renal calculi, including the development of nephrostomy tract balloon dilators, improved grasping instruments, and the use of improved methods of stone fragmentation and removal [6,7].
The nephrostomy tract is usually performed as a “single stage procedure” under the same general anaesthetic as percutaneous stone removal. The procedure involves the following sequential steps:
Under a general anaesthetic, with the patient in a supine position, a retrograde ureteral catheter is placed using a cystoscope.
After turning the patient to a prone position, the renal collecting system is accessed via an 18 gauge needle under fluoroscopic guidance.
After dilation of the tract to 32F with a nephrostomy balloon dilator, a 30F working sheath is placed into the renal collecting system.
All calculi are extracted with grasping forceps using a rigid and/or flexible nephroscope, and/or fragmented using an ultrasonic, pneumatic, or combined ultrasonic/pneumatic lithotripsy probe using a rigid nephroscope.
Following successful stone removal, it is standard to leave a large nephrostomy tube and a urethral
catheter.
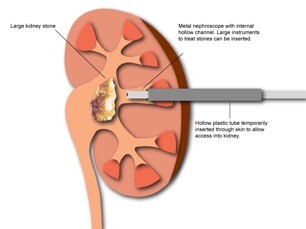
Figure 1. Schematic representation of large renal stone being removed by PCNL.
Side Effects associated with PCNL
Common (greater than 1 in 10)
Temporary insertion of a bladder catheter and ureteric stent/ kidney tube needing later removal
Transient blood in the urine
Transient raised temperature
Occasional (between 1 in 10 and 1 in 50)
Occasionally more than one puncture site is required
No guarantee of removal of all stones & need for further operations
Recurrence of new stones
Failure to establish access to the kidney resulting in the need for further surgery
Rare (less than 1 in 50)
Severe kidney bleeding requiring transfusion, embolisation or at last resort surgical removal of kidney. Damage to lung, bowel, spleen, liver requiring surgical intervention.
Kidney damage or infection needing further treatment
Over-absorption of irrigating fluids into blood system causing strain on heart function
SHOCK WAVE LITHOTRIPSY
The development of extracorporeal shock wave lithotripsy (ESWL) was a significant advance related to the removal of renal and ureteral stones. However, ESWL is not the ideal modality for the management of large or complex calculi. Alternative modes of stone removal should be considered for large or hard calculi, stones located in a calyceal diverticulum, or in patients with complex renal anatomy. Procedures such as percutaneous stone removal or a ureteroscopic approach can greatly facilitate stone removal and correct underlying anatomic abnormalities [12-14]. In studies with renal calculi measuring 11 to 20 mm in diameter, single treatment success
rates were significantly better in those who underwent percutaneous stone removal (95 percent) and ureteroscopy
(88 percent) compared with SWL (60 percent) [15].
ESWL employs high energy shock waves produced by an electrical discharge. The shock waves are transmitted through water and directly focused onto a renal/ureteral stone with the aid of biplanar fluoroscopy. The change in tissue density between the soft renal tissue and the hard stone causes a release of energy at the stone surface. This energy fragments the stone.
While current lithotriptor technology is quite effective in fragmenting the majority of renal and ureteral calculi, there continues to be some debate concerning the potential deleterious effects of the high-energy shock waves, such as hypertension, renal injury, and, in men, sperm DNA damage and a temporary decline in fertility [16-18].
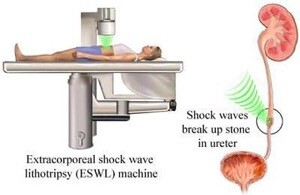
Figure 3. Schematic representation of how ESWL works
Side Effects of ESWL
Common (greater than 1 in 10)
Bleeding on passing urine for a short period after the procedure
Pain in the kidney as small fragments of stone pass after treatment (20%)
Urinary tract infection due to bacteria released from the stone during fragmentation, requiring antibiotic treatment (10%)
Bruising or blistering of the skin in the loin or on the front of the abdomen
Need for repeated ESWL treatments (15-20%)
Failure to fragment very hard stone(s) requiring an alternative treatment (less than approximately 14%)
Occasional (between 1 in 10 and 1 in 50)
Severe infection requiring intravenous antibiotics (less than 1%) and sometimes drainage of the kidney by a small drain placed through the back into the kidney
Stone fragments occasionally get stuck in the tube between the kidney and the bladder requiring hospital attendance and, occasionally, surgery to remove the stone fragments
Rare (less than 1 in 50)
Kidney damage (bruising) or infection needing further treatment
Recurrence of stones (less than 1%)
OPEN STONE SURGERY
There continues to be a limited role for open stone surgery. Less than one percent of patients are candidates for such surgery.
Open stone surgery is primarily reserved for the management of complex renal and ureteral calculi that cannot be removed with a reasonable number of minimally invasive procedures. Current indications include patients who have failed endoscopic stone removal, patients with complex (staghorn) renal calculi, and patients with complex renal/ureteral anatomy or morbidly obesity [14].
REFERENCES
- 1. Preminger GM, Clayman RV, Hardeman SW, et al. Percutaneous nephrostolithotomy vs open surgery for renal calcu A
comparative study. JAMA 1985; 254:1054.
- 2. Jewett MA, Bombardier C, Menchions C Comparative costs of the various strategies of urinary stone disease management.
Urology 1995; 46:15.
- 3. Grasso M, Beaghler M, Loisides P. The case for primary endoscopic management of upper urinary tract calculi: II. Cost and outcome assessment of 112 primary ureteral calcu Urology 1995; 45:372.
- 4. Meretyk S, Gofrit ON, Gafni O, et al. Complete staghorn calculi: random prospective comparison between extracorporeal shock wave lithotripsy monotherapy and combined with percutaneous nephrostolithotom J Urol 1997; 157:780.
- 5. Al-Otaibi K, Hosking D Percutaneous stone removal in horseshoe kidneys. J Urol 1999; 162:674.
- 6. Pietrow PK, Auge BK, Zhong P, Preminger Clinical efficacy of a combination pneumatic and ultrasonic lithotrite. J Urol
2003; 169:1247.
- 7. Auge BK, Sekula JJ, Springhart WP, et al. In vitro comparison of fragmentation efficiency of flexible pneumatic lithotripsy using 2 flexible ureteroscope J Urol 2004; 172:967.
- 8. Segura JW, Preminger GM, Assimos DG, et Ureteral Stones Clinical Guidelines Panel summary report on the management of ureteral calculi. The American Urological Association. J Urol 1997; 158:1915.
- 9. Kourambas J, Munver R, Preminger GM. Ureteroscopic management of recurrent renal cystine calcu J Endourol 2000;
14:489.
- 10. Kourambas J, Delvecchio FC, Munver R, Preminger GM. Nitinol stone retrieval-assisted ureteroscopic management of lower pole renal calculi. Urology 2000; 56:935.
- 11. Auge BK, Dahm P, Wu NZ, Preminger GM. Ureteroscopic management of lower-pole renal calculi: technique of calculus displacem J Endourol 2001; 15:835.
- 12. Streem Contemporary clinical practice of shock wave lithotripsy: a reevaluation of contraindications. J Urol 1997;
157:1197.
- 13. Streem SB, Yost A, Dolmatch Combination “sandwich” therapy for extensive renal calculi in 100 consecutive patients:
immediate, long-term and stratified results from a 10-year experience. J Urol 1997; 158:342.
- 14. Matlaga BR, Assimos D Changing indications of open stone surgery. Urology 2002; 59:490.
- 15. Wiesenthal JD, Ghiculete D, D’A Honey RJ, Pace A comparison of treatment modalities for renal calculi between 100 and
300 mm2: are shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy equivalent? J Endourol 2011; 25:481.
- 16. Gupta M, Bolton DM, Irby P 3rd, et al. The effect of newer generation lithotripsy upon renal function assessed by nuclear scintigraphy. J Urol 1995; 154:947.
- 17. Krambeck AE, Gettman MT, Rohlinger AL, et Diabetes mellitus and hypertension associated with shock wave lithotripsy of renal and proximal ureteral stones at 19 years of followup. J Urol 2006; 175:1742.
- 18. Gulum M, Yeni E, Kocyigit A, et al. Sperm DNA damage and seminal oxidative status after shock-wave lithotripsy for distal ureteral ston Fertil Steril 2011; 96:1087.
If you’d like to find out more information or request an appointment with our urology clinic in Berkshire or Windsor, please get in touch using our contact form available on the website or call 017 53 66 5415.









