HoLEP Treatment in Windsor & Berkshire
Private Holmium Laser Enucleation of the Prostate Treatment (HoLEP)
INTRODUCTION TO HoLEP
Benign prostatic hyperplasia (BPH) is a condition that presents when the prostate gland enlarges, potentially slowing or blocking the urine stream. The most common symptoms include needing to urinate frequently (during the day and night), a weak urine stream, and leaking or dribbling of urine. These symptoms are called lower urinary tract symptoms (LUTS). For men with bothersome or severe symptoms, treatment with surgery is an option. Mr Kalsi is a national mentor and trainer in the new gold standard laser treatment option (HoLEP)
THE PROSTATE GLAND
The prostate is a small gland that is part of the male reproductive system. It sits just below the bladder and in front of the rectum (Figure 1). The prostate is normally about the size of a walnut. The prostate is composed of two lobes, covered by an outer layer of tissue. The prostate surrounds the urethra, the tube that carries urine from the bladder through the penis and outside the body.
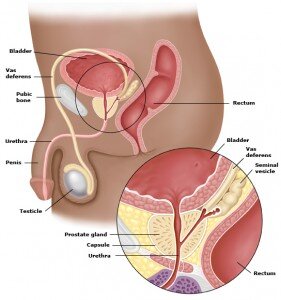
Figure 1. Demonstrating the male anatomy and a close-up of the prostate gland.
SURGICAL TREATMENTS
If medicines do not relieve your symptoms of BPH, a surgical treatment may be recommended. Other indications for surgery include:
- High pressure retention of urine (where there has back pressure to your kidneys)
- Acute retention of urine which is not reversible (refractory) or is recurrent,
- Complications from a large prostate gland or incomplete bladder emptying such as recurrent haematuria (blood in the urine, urinary tract infections (UTIs) and bladder stones.
Surgery is used to reduce to reduce the amount of prostate tissue around the urethra (figure 1). The new gold standard treatment involves using a Holmium laser (Holmium laser enulcleation of the prostate or HoLEP).
HOLMIUM LASTER ENUCLEATION OF THE PROSTATE (HoLEP)
This procedure is done in a very similar way to a standard TURP and is now considered to be the new Gold Standard [1]. Rather than using heat diathermy, a Holmium laser is used to separate the obstructing prostate tissue from its surrounding capsule and to push the large prostate chunks into the bladder (Figure 2). A special instrument (morcellator) is then used through the telescope to remove the prostate tissue from the bladder [7,8]. A catheter is normally left to drain the bladder at the end of the procedure. This technique can be employed for prostates of any size [4] and is the only laser technique recommended by NICE and where tissue can be preserved for histology analysis. This technique has a much lower risk of post-operative bleeding. The urine is usually clear of blood after 12 hours, although some patients lose more blood for longer. It is unusual to require a blood transfusion after laser surgery (1% vs 7% for TURP). Other advantages include a lower risk of bladder neck or urethral strictures (4% vs 8%), a significant reduction in in-patient stay (1 vs 2.5 nights) and no risk of TUR syndrome (Absorption of irrigating fluids causing confusion) [5].
The catheter is generally removed early the next morning after surgery. This allows your bladder to fill and allow the medical team to decide whether you may go home without the catheter. At first, it may be painful to pass your urine and it may come more frequently than normal. Any initial discomfort can usually be relieved by tablets and the frequency usually improves within a few days. Some of your symptoms, especially frequency, urgency and getting up at night to pass urine, may not improve for several months because these are often due to bladder over-activity (which takes time to resolve after prostate surgery) rather than prostate blockage. Since a large portion of prostate tissue is removing with the laser technique, there may be some temporary loss of urinary control (incontinence 1-3%) until your pelvic floor muscles strengthen and recover [6]. In certain cases this operation may be carried out on patients on Asprin or other forms of anticoagulation.

Figure 2. Intra-operative picture of Mr Kalsi performing a Holmium laser enucleation (HoLEP)
SIDE EFFECTS
Common (greater than 1 in 10)
- Temporary mild burning, bleeding and frequency of urination after the procedure
- No semen is produced during an orgasm in approximately 75% (Retrograde ejaculation)
- Treatment may not relieve all the prostatic symptoms
- Poor erections (impotence in approximately 5-10%)
- Infection of the bladder, testes or kidney requiring antibiotics
- Possible need to repeat treatment later due to re-obstruction (approx 10%)
Occasional (between 1 in 10 and 1 in 50)
- Injury to the urethra or bladder neck causing delayed scar formation (4-8%)
- Bleeding requiring return to theatre and/or blood transfusion (1%)
- Finding unsuspected cancer in the removed tissue which may need further treatment
- May need self-catheterisation to empty bladder fully if the bladder is weak
- Failure to pass urine after surgery requiring a new catheter
- Loss of urinary control (incontinence) which may be temporary or permanent (2-4%)
- Rare (less than 1 in 50)
- Very rarely, perforation of the bladder requiring a temporary urinary catheter or open surgical repair
REFERENCES
1. Elzayat EA, Habib EI and Elhilali MM: Holmium laser enucleation of the prostate: a size-independent new ‘gold standard’. Urology 2005; 66: 108.
2. Gilling PJ, Aho TF, Frampton CM et al: Holmium laser enucleation of the prostate: results at 6 years. Eur Urol 2008; 53: 744.
3. Elzayat EA, Habib EI and Elhilali MM: Holmium laser enucleation of prostate for patients in urinary retention. Urology 2005; 66: 789.
4. Kuntz RM, Lehrich K and Ahyai SA: Holmium laser enucleation of the prostate versus open prostatectomy for prostates greater than 100 grams: 5-year follow-up results of a randomised clinical trial. Eur Urol 2008; 53: 160.
5. Ahyai SA, Lehrich K and Kuntz RM: Holmium laser enucleation versus transurethral resection of the prostate: 3- year follow-up results of randomized clinical trial. Eur Urol 2007; 52: 1456.
6. Anderson CB, Helfand BT and McVary KT: Holmium laser prostatic resection for patients presenting with acute urinary retention. BJU Int 2008; 102: 1623.
7. Vavassori I, Valenti S, Naspro R et al: Three-year outcome following holmium laser enucleation of the prostate combined with mechanical morcellation in 330 consecutive patients. Eur Urol 2008; 53: 599.
8. Baazeem A, Elmansy H and Elhilali M: Holmium laser enucleation of the prostate: modified technical aspects. BJU Int 2010; 105: 584.
9. Elmansey H. Holmium laser enucleation of the prostate:
If you’d like to find out more information about HoLEP treatments offered by Jas Kalsi or request an appointment with our urology clinics in Berkshire or Windsor , please get in touch using our contact form available on the website or call 017 53 66 5415.









