Male infertility can be a tragic and frustrating situation for couples wishing to conceive a child. For men who have no sperm present in the ejaculate (Azoospermia), help can be found in the hands of a private urologist experienced microsurgeons, such as Mr Jas Kalsi. Using state–of–the–art microsurgical technology, patients can be sure they are receiving some of the most effective male infertility care currently available.
Mr Jas Kalsi – Consultant Urological Surgeon is highly trained and experienced in male reproductive medicine and surgery.
Mr Kalsi’s approach to problem solving is sensitive and friendly. He is highly skilled at performing microsurgical sperm retrieval from either the epididymis (MESA) or from the testis (m-TESE). His meticulous microsurgical technique results in successful sperm retrieval in a high number of cases even when there has been previous failed surgery elsewhere. He is among a very limited group of micro surgeons in the UK who can perform the newer technique of sperm retrieval from the testes called micro-dissection TESE (m-TESE) which results in a higher success rate of positive sperm retrieval whilst minimising the amount of tissue taken and potentially damage to the testis
Mr Kalsi graduated from from University College and Middlesex School of Medicine with Honours. He completed his Urology training on the Imperial higher surgical scheme in London and completed his Fellowship in Andrology and Male Reproductive Medicine and Surgery at The Institute of Urology, University College London. He has also authored several peer reviewed journal articles and several chapters regarding treatments for male infertility. He is also a media spokesperson on male health issues including male sexual dysfunction and infertility.
As a sub-specialist, Mr Kalsi also treats a wide range of other problems related to male infertility and sexual dysfunction. He provides the comprehensive evaluation and care that men in infertile couples deserve and require. The process begins with a thorough physical examination, accompanied by a medical and fertility history. The inability to father a child can be caused by a number of conditions, including chronic disease, injuries, childhood illnesses, congenital conditions, hormone deficiencies, smoking and other lifestyle choices, medications and pelvic surgery involving structures such as the prostate gland and reproductive organs. If you need any further information please email info@urologynow.co.uk
Non-Obstructive azoospermia
Historically, the management of azoospermia is by assessment of the male partner with a hormonal assay and genetic analyses. As endocrine tests cannot always distinguish normal (Obstructive azoospermia, OA) from impaired spermatogenesis (Non-Obstructive Azoospermia, NOA) or predict retrieval of mature sperm for ICSI,
in the UK an isolated diagnostic testicular biopsy is commonly sent for histopathological confirmation of sperm production before sperm retrieval is attempted (1). However, It is now well accepted that although histopathology may suggest no active sperm production, within each testis, there may well be small isolated areas of sperm production within the testis (2). Three techniques are currently available for testicular sperm retrieval. Testicular exploration and sperm extraction (TESE) with multiple biopsies is currently the most frequently used technique. However this involves the removal of large samples of testicular tissue in an attempt to improve retrieval rates over a single biopsy (7).
In contrast, the fine needle aspiration (FNA) offers a less invasive approach. However, its efficacy in NOA is lower than that of TESE (8). The micro-dissection (m-TESE) technique was developed to combine the advantages of an open excision technique without the need to remove large quantities of testicular tissue (5).
Many studies have suggested that the micro-dissection (m-TESE) sperm retrieval is now the gold standard technique in management of men with NOA (3;4). Sperm retrieval with m-TESE has revolutionised the management of men with NOA with sperm retrieval rates of between 40-60% being achieved in a number of studies (5). The procedure appears to be safe resulting in minimal complications but with a higher yield of sperm retrieval (4). At the same time as the sperm retrieval, a small biopsy is sent for histopathology and reported using the scoring system for spermatogenesis is that proposed by Johnsen (1970) (6). A recent UK study has reported that sperm retrieval can be expected in up to 50% of cases irrespective of the underlying histology. The term ‘sertoli cell only (SCO) is used if all the tubules in the biopsy show a total absence of germ cells (1). Where tubules containing sertoli cells are found in the same biopsy in which other tubules contain more advanced spermatids, the diagnosis is hypospermatogenesis (1). In this case all stages of spermatogenesis are present but reduced to a varying degree (Johnsen score < 8). Maturation arrest describes the total arrest at a particular stage, most commonly at the spermatogonial or primary spermatocyte stage. There is no progression seen beyond this stage in any tubule in the entire biopsy (Johnsen score < 5) (1). If there are even small numbers of spermatids seen in a single tubule in a biopsy where the rest of the tubules contain only primary spermatocytes, the term maturation arrest should not be used. In this case the term severe hypospermatogenesis is more appropriate
Retrieval of sperm from the testis (m-TESE)
The newer surgical technique to retrieve spermatozoa from patients with non-obstructive azoospermia [90] called micro-dissection TESE (m-TESE) has been successful in obtaining sperm in over 50 percent of patients with non-obstructive azoospermia, including patients with Klinefelters syndrome (9,10). This technique requires considerable expertise and should only be performed in a centre where the urologist has been trained and is skilled in these procedures. This technique may also be successfully used in men who become azoospermic post-chemotherapy. Ideally, men who will be undergoing chemotherapy should be referred for sperm banking. However, studies from the USA show that only 50 per cent are offered this option and even fewer have successfully frozen sperm (11). In the past, men who developed azoospermia after chemotherapy were considered to be sterile. Now, many of these men (approximately 37 percent in one study) are able to undergo successful testicular sperm extraction and intracytoplasmic sperm injection (12).
The Technique
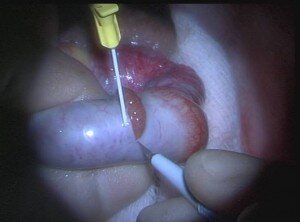
Under a general anaesthesia, a mid-line scrotal incision is made on the median raphe of the scrotum delivering both testes. A transverse or equatorial incision is then made under magnification avoiding the vessels on each testis (Figure 1). The underlying sub- tunical vessels are preserved and using an operating microscope at x25 magnification, tubular dissection is performed (Figure 2). Using the operative microscope opaque and more dilated tubules are gently removed and immediately placed within a sperm buffer such as Quinn’s Advantage Fertilisation Medium (Sage Inc, Trumbull USA). Using high powered ICSI microscopes (x 200) the tubules are immediately dissected by an embryologist. If sperm is successfully obtained this can be either frozen or used for injection for a concurrent cycle of ICSI. Recent studies have shown that frozen sperm is likely to be as good as fresh sperm when used in cycles of Intracytoplasmic sperm injection (ICSI) (13). At the same time as performing a micro-dissection sperm retrieval, biopsies are also sent for histopathological examination. The patients were usually discharged on the day of surgery with analgesia and prophylactic antibiotics usually given for 7 days. The patients are then followed up in outpatients in 2 weeks and then again in 6 months with a hormonal assay.
Figure 1. After the testis is delivered, a transverse or equatorial incision was made to avoid the subtunical vessels.
Figure 2. Using an operating microscope at x25 magnification tubular dissection is undertaken of the most dilated and opaque tubules.
Side Effects
Common (greater than 1 in 10)
Future fertility cannot be guaranteed
If storing tissue, check that the appropriate forms have been signed
Bruising and swelling of the scrotum/testes
Occasional (between 1 in 10 and 1 in 50)
Infection of the incision requiring further treatment
Inconclusive diagnosis from the biopsy
Rare (less than 1 in 50)
Damage to the testicle, epididymis or vas from biopsy
Shrinkage (atrophy) of the testis and hypogonadism
Chronic pain in the testicle or scrotum
References
1. McLachlan RI, Rajpert-De ME, Hoei-Hansen CE, de Kretser DM, Skakkebaek NE. Histological evaluation of the human testis–approaches to optimizing the clinical value of the assessment: mini review. Hum Reprod 2007 Jan;22(1):2-16. 2. Haimov-Kochman R, Lossos F, Nefesh I, Zentner BS, Moz Y, Prus D, et al. The value of repeat testicular sperm retrieval in azoospermic men. Fertil Steril 2009 Apr;91(4 Suppl):1401-3. 3. Kalsi JS et al. In the era of micro-dissection sperm retrieval (m-TESE) is an isolated testicular biopsy necessary in the management of men with non-obstructive azoospermia? BJUInt 2012 Feb 109(3):418- 24. 4. Amer M, Ateyah A, Hany R, Zohdy W. Prospective comparative study between microsurgical and conventional testicular sperm extraction in non-obstructive azoospermia: follow-up by serial ultrasound examinations. Hum Reprod 2000 Mar;15(3):653-6. 5. Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision. Hum Reprod 1999 Jan;14(1):131-5. 6. de Kretser DM, Burger HG, Fortune D, Hudson B, Long AR, Paulsen CA, et al. Hormonal, histological and chromosomal studies in adult males with testicular disorders. J Clin Endocrinol Metab 1972 Sep;35(3):392-401. 7. Tournaye H, Liu J, Nagy PZ, Camus M, Goossens A, Silber S, et al. Correlation between testicular histology and outcome after intracytoplasmic sperm injection using testicular spermatozoa. Hum Reprod 1996 Jan;11(1):127-32. 8. Friedler S, Raziel A, Strassburger D, Soffer Y, Komarovsky D, Ron-El R. Testicular sperm retrieval by percutaneous fine needle sperm aspiration compared with testicular sperm extraction by open biopsy in men with non-obstructive azoospermia. Hum Reprod 1997 Jul;12(7):1488-93. 9. Schiff JD, Palermo GD, Veeck LL, et al. Success of testicular sperm extraction [corrected] and intracytoplasmic sperm injection in men with Klinefelter syndrome. J Clin Endocrinol Metab 2005; 90:6263. 10. Schlegel PN. Nonobstructive azoospermia: a revolutionary surgical approach and results. Semin Reprod Med 2009; 27:165. 11. Schover LR, Brey K, Lichtin A, et al. Knowledge and experience regarding cancer, infertility, and sperm banking in younger male survivors. J Clin Oncol 2002; 20:1880. 12. Hsiao W, Stahl PJ, Osterberg EC, et al. Successful treatment of postchemotherapy azoospermia with microsurgical testicular sperm extraction: the Weill Cornell experience. J Clin Oncol 2011; 29:1607. 13. Kalsi JS et al. Analysis of the outcome of intra-cytoplasmic sperm injection using fresh or frozen sperm. BJU Int 2011 April 107(7):1124-8