Peyronie’s disease
Peyronie’s disease can present with penile pain, penile shortening, penile deviation and worsening erectile function. Often the features can be very subtle and diagnosis may be delayed causing significant distress to the patient. However, help can be found in the hands of experienced andrological surgeons such as Mr Jas Kalsi. Using state–of–the–art surgical technology, patients can be sure they are receiving some of the most effective care currently available including the latest options such as injections with Collagenase (Xiapex).
Mr Jas Kalsi – Consultant Urological Surgeon is highly trained and experienced in male sexual medicine (Andrology) and surgery.
Mr Kalsi’s approach to problem solving is sensitive and friendly. He is highly skilled at performing all types of medical and surgical treatments for Peyronie’s and erectile dysfunction (ED). His meticulous surgical technique results in successful surgery, including cases of previous failed treatment elsewhere. He has also authored several peer reviewed journal articles and several chapters regarding treatments for Peyronie’s disease and erectile dysfunction. He is also a media spokesperson on male health issues. As a sub-specialist, Mr Kalsi provides the comprehensive evaluation and care that men with andrological problems deserve and require. The process begins with a thorough physical examination, accompanied by a medical and sexual history.
INTRODUCTION
Peyronie’s disease, an acquired, localized fibrotic disorder of the tunica albuginea, can cause significant penile deformity and lead to sexual dysfunction and psychological trauma (figure 1). The nature and extent of Peyronie’s plaque, and therefore severity or complexity of penile deformity, varies widely.
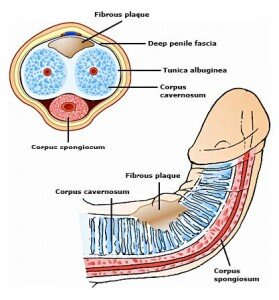
Figure 1. Peyronie’s disease is an acquired, localized fibrotic disorder of the tunica albuginea causing
penile deformity.
MEDICAL TREATMENT
The optimum medical therapy for Peyronie’s disease (PD) has not yet been identified. A number of different options have been investigated.
Oral preparations
The antioxidant vitamin E has been used since 1948 because of its low incidence of adverse effects and low cost. In 1993, it was reported that there was a 99% reduction in pain and a 13% reduction in penile curvature, even though 70% of the patients were found to have no objective change in their symptoms
Another oral agent that has had varied success in treating this condition is potassium aminobenzoate ([PABA] Potaba). In a retrospective study, it was found that there was a decrease in penile plaque size in 18 of 32 patients and a resolution of penile angulation in 18 of 31 patients treated with 12 g of PABA daily for at least 3 months. Unfortunately, therapy requires an excessive amount of PABA to be taken each day for a usual 6-month course. Most patients find the adverse gastrointestinal effects to be intolerable.
Other options that have been investigated include the nonsteroidal antiestrogen tamoxifen and the anti-inflammatory agent colchicine, with limited success.
Injection therapy
This option has gained considerable interest in the last 12 months. Intralesional injection of various substances has been used for decades in an attempt to dissolve the plaques of PD. Various steroid preparations have been used (dexamethasone, triamcinolone hexacetonide, betamethasone) with studies suggesting minimal benefit over placebo.
However the recent licence for Collagenase clostridium histolyticum (Xiapex) in the UK has resulted in growing interest in injectable treatment as an option for both the acute and chronic phase. Xiapex is an injectable proteinase that hydrolyzes collagen in its native triple-helical conformation, resulting in lysis of collagen deposits. This is now also fully licenced in the USA by the FDA. It is recommended to be used in up to 4 treatment cycles along with penile stretching.
Xiapex is indicated for the treatment of adult men with Peyronie’s disease with a palpable plaque and curvature deformity of at least 30 degrees at the start of therapy. It is very important that Xiapex is administered by a specialist who is appropriately trained and registered such as Mr Kalsi.
A treatment course consists of a maximum of 4 treatment cycles. Each treatment cycle consists of 2 Xiapex injection procedures and one in-clinic penile modeling procedure. The second Xiapex injection procedure occurs 3-5 days after the first. The in-clinic penile modeling procedure is performed 3-5 days after the second injection of the treatment cycle. The injection may be performed under local anaesthetic when you are awake or under general ie asleep. Improvement in curvature >20 degrees is seen in up to 60% of patients.
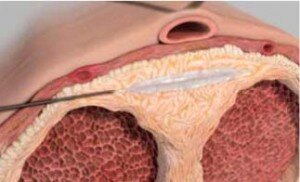
The tip of the needle placed within the plaque, then the drug is slowly injected into the plaque
Until the recent licence for Xiapex in the UK, the most popular injectable treatment for Peyronies disease was Verapamil. Verapamil is a calcium channel blocker that has gained attention for the treatment of PD since it was found that it induced increased collagenase activity. Levine et al first published results of the use of intralesional verapamil for PD in an uncontrolled study in 1994. These authors reported reduced pain in 93% of men treated with 10 mg of verapamil injected intralesionally. They also noted 100% subjective improvement in hourglass deformity, 42% objective improvement in curvature, and 58% improvement in ED. The best outcomes were achieved when used in 20ml dilutions every 2 weeks over a 6 week period. Mr Kalsi recommends this treatment option along with the use of a vacuum device.
External vacuum and other mechanical devices
External vacuum devices have been used to attempt to stretch the scarred areas through mechanical means. The patient is instructed to apply the vacuum cylinder and inflate it to maximal tolerable pressure for 10-15 minutes. No tension ring or band is applied. This procedure is repeated once or twice a day for several months. Various studies have shown promising results on a short term basis.
Levine and Newell (2008) reviewed the use of the FastSize Medical Extender in the treatment of PD. This mechanical device uses controlled periodic stretching of the flaccid penis to extend the length and, in the case of PD, to hopefully straighten the curvature of the penis. They found that significant (10°-45°) improvement in curvature could be achieved in small clinical trials and recommended that larger-scale trials using this device are justified. The long-term benefits and limitations of this new device are pending further trials.
Gontero et al (2009) investigated a similar penile extender, the Andropenis (Andromedical, Madrid, Spain), in a phase II prospective study of 15 patients. Men with stable PD, mild penile curvature (not exceeding 500 ), and mild to no ED were studied. They were required to wear the device for at least 5 hours per day for 6 months. These authors found that this device provided only minimal improvement in penile curvature (average 310 at start to 270 at end). The mean stretched penile length increased by 1.3 cm over the study period and is probably why the satisfaction rate was favorable. This therapy may be beneficial in selected patients with minimal curvature and little to no associated ED, but its ability to straighten a curved penis requires further investigation.
SURGICAL INDICATIONS
Surgical management is indicated for patients whose Peyronie’s disease has persisted for more than 6-12 months and is associated with a penile deformity compromising sexual function. It is important to delay surgery until Peyronie’s disease has been stable for at least three months because surgical results can be compromised by active disease [1,2].
Surgery is not indicated for plaque without curvature, or minimal degrees of curvature. The main determinant is whether sexual intercourse without pain is possible [3]. Curvature that does not preclude intercourse does not warrant surgery.
Concurrent implantation of a penile prosthesis is indicated in men with Peyronie’s disease and erectile dysfunction (ED) unresponsive to oral agents or intracavernous injection therapy.
PREOPERATIVE EVALUATION
A thorough review of the patient’s medical and surgical history and a physical examination are performed. Medications that prolong bleeding, such as aspirin, are generally discontinued 7 to 10 days prior to the procedure.
MRI or Duplex ultrasound evaluation of erectile capacity
A preoperative penile MRI or duplex ultrasound combined with intracavernous injection of a vasoactive agent is performed if distal flaccidity is present, or erectile function is in question. Ultrasound assesses the nature and location of the Peyronie’s plaque and penile vascular anatomy, identifying any arterial and/or venous components of erectile dysfunction, if present. This information is particularly useful if grafting is being considered. MRI is used to identify the degree of curvature, the size and position of the plaque and whether there are any complex features such as an hourglass deformity or a hinge defect
Preoperative penile photographs/measurements
Preoperative penile photographs are usually obtained of the erect penis to document penile length, nature (dorsal, ventral lateral), and degree of curvature for future reference.. Photographs in multiple views can be taken by the patient at home, or in the outpatients’ by inducing an artificial erection by injecting a vasodilating medication, such as Caverject (alprostadil).
Choice of surgical approach
The most important factor determining surgical success is selection of the appropriate surgical procedure for a given patient. Surgical options include tunical shortening (eg, plication), tunical maintaining (eg, grafting) or implantation of penile prostheses.
Important factors to consider in determining the best surgical approach include the length of the penis, configuration (eg, hourglass, curved) and severity of the deformity, erectile capacity, and patient expectations [2,4].
- For a penis with a simple curvature <60 degrees, adequate length, and intact erectile function, a tunical shortening procedure (ie, tunica wedge resection, plication) technique is appropriate. This procedure will not correct an hourglass deformity or hinge effect. When performed on appropriately selected men, simplified tunical shortening (ie, pure plication) offers satisfactory results and minimizes surgical morbidity.
- For a very short penis, the presence of a severe curvature (>60º), narrowing deformity (eg, hourglass, severe indentation), and good erectile function, tunical maintaining with plaque incision and graft placement may restore penile length, and/or girth.
- For curvature associated with significant ED, a penile prosthesis can be placed and additional corrective procedures (plication or grafting) are performed if the prosthesis does not provide adequate straightening
Patient counselling
A thorough preoperative discussion is essential and should review preparation, complications and realistic longterm outcomes associated with the planned surgery. Patients are fully informed of the risks of reduced temporary or permanent penile sensation, future plaque formation, recurrent curvature, and risk of de novo or worsened ED.
If erectile function is compromised preoperatively, the risk of further dysfunction is increased. Patients with a history of cardiovascular disease (ie, coronary artery disease [CAD] or peripheral artery disease [PAD]), diabetes, or smoking also have an increased long-term risk for ED, independent of the surgery performed for Peyronie’s disease [5].
Patients with ED or significant risk factors for future ED should be counselled regarding the placement of a penile prosthesis at the time of surgery. Prostheses may also be placed at a later date as the need arises.
Patient expectations about postoperative penile length should also be addressed. Penile shortening often accompanies Peyronie’s disease and is dependent on direction and degree of curvature, and original penile length [6]. Patients, however, may have unrealistic recollections of their erect penile length prior to the onset of Peyronie’s disease, and premorbid penile measurements are rarely available. The patient is informed that plication surgery may result in a straight erection but is not likely to restore any length, and in fact will likely reduce length. With tunical maintaining procedures (ie, grafting), only about 1/2 to 1 inch of additional length can be expected. It is important to document and review the preoperative stretched penile length with the patient.
We do not routinely remove the foreskin at the time of surgery. However, if the foreskin is tight either at the beginning of surgery or at the end then a circumcision is performed to prevent foreskin necrosis, which can be difficult to manage. Only 20-30% of patients require a circumcision.
GENERAL APPROACH
Reconstructive procedures for Peyronie’s disease are usually performed with an overnight hospital stay, an insertion of a urethral catheter and under a general anaesthetic.
Prior to the incision, intravenous antibiotics are given. The patient is positioned supine and the operative area depilated with a clipper. Bladder drainage is performed with a urethral catheter.
Following sterile preparation, an artificial erection is induced by injecting normal saline into the corpus cavernosum; this aids in pre-procedure planning and intraoperative assessment of surgical results. The site of greatest curvature and plaque is marked and a circumferential incision made below the glans penis. The penis is then de-gloved to access the tunica albuginea.
TECHNIQUES
Plication
Straightening the penis with plication is achieved by shortening the convex side of the penis (ie, opposite the plaque) and should only be performed in men with adequate penile length and curvature less than 60º (figure 2). All plication procedures result in loss of penile length as the tunica albuginea is shortened on the longer side to match the shorter side [6].
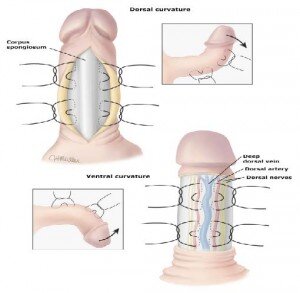
Figure 2. Straightening the penis with plication is achieved by shortening the convex side of the penis (ie,
opposite the plaque). Plication is generally performed in men with adequate penile length.
Soft, delayed absorbable sutures are used because they are the least noticeable under the skin.
When the tunica albuginea is plicated without incision (ie, pure plication), normal anatomy is minimally disrupted. Since dorsal curvature is the most prevalent, plication of the ventral surface avoids the need to dissect the dorsal neurovascular bundle.
The most common plication techniques are:
- Nesbit procedure – One or more ellipses of the tunica albuginea are excised from the convex side (ie,
tunica wedge resection) and the tunica plicated at the most prominent portion of the curvature [8]. •Yachia procedure – Longitudinal incisions in the tunica albuginea on the convex side are closed horizontally (eg, Heineke-Mikulicz) [9].
- The 16 dot technique – This is a pure plication procedure consisting of two or three pairs of plications on the convex side [10,11]. Paired, mattress sutures are placed in the tunica albuginea and tension adjusted to straighten the curvature prior to completing the ties.
Grafting
Men with Peyronie’s disease who have a short penis, extensive plaque, severe (>60º), or complex deformities will require a grafting procedure. Grafting the concave side of the penis serves to lengthen that side and, therefore, straighten the penis (figure 3).
Opening the tunica albuginea often worsens erectile function. Patients must be aware of this risk, and should be counselled regarding the option of penile prosthesis implantation [12].
Graft materials
Following management of the plaque, a graft is placed. The choice of graft material depends upon several factors, including type of deformity, efficacy, and availability [13]. Grafting materials include:
- Autologous tissue (eg, saphenous vein, fascia lata, rectus fascia, tunica vaginalis, dermis, buccal mucosa).Vein patch is the most commonly used autograft material and is harvested from the distal saphenous vein; if a larger graft is needed, the proximal saphenous vein can be used. Saphenous vein is spared in patients with significant cardiovascular disease (ie, CAD, PAD); these patients may need the
saphenous vein for future bypass grafting.
- Allograft or xenograft materials (eg, engineered dermal graft (Pelvicol), cadaveric or bovine pericardium, porcine small intestinal submucosa [SIS]) [14-16]. These acellular matrices allow regenerative ingrowth of native tissues. The main advantage of allograft tissues is elimination of the need for tissue
harvesting.
Penile prosthesis
The treatment of choice for patients with Peyronie’s disease and significant ED is placement of a penile prosthetic implant with or without manual modelling and with or without penile reconstruction. Patient satisfaction is higher with inflatable penile prostheses than malleable devices (Figure 4) [1,17].

Figure 4. A Three piece inflatable penile prosthesis consisting of a reservoir, a pump and 2 cylinders.
The correction of penile curvature can be accomplished solely by implantation of the penile prosthesis in patients with mild to moderate curvature. Manual modelling over the prosthesis may be required to correct more significant deformities (eg, >30º curvature) [18]. Penile reconstruction (plaque incision/grafting) can be performed before or after implant placement in patients with severe or complex deformities, or calcified Peyronie’s plaque [19].
Manual modelling is a process by which the tunica plaque is fractured over the inflated prosthetic cylinder at the time of implantation. The penis is forcibly bent in a direction opposite the curvature [18]. Bending pressure is maintained on the penis for 90 seconds. When successful, the modeling procedure causes splitting and rupturing of the fibrotic plaques. The penile implant is left partially inflated for six weeks to prevent contraction of the tunica defect which could lead to recurrent curvature.
Side Effects associated with Penile Straightening surgery
Common (greater than 1 in 10)
There will be some shortening of the penis by 1-2cm, (especially with Nesbit’s procedure but also to a lesser degree with the Lue procedure) in addition to the shortening already produced by the disease itself
Possible dissatisfaction with the cosmetic or functional result with a residual curvature; generally, any recurrent or residual curve does not require further surgery
Temporary swelling and bruising of the penis and scrotum lasting several days
Stitches under the skin which you may be able to feel
Circumcision is sometimes required as part of the procedure
Insertion of a catheter into the bladder is often necessary
Occasional (between 1 in 10 and 1 in 50)
No guarantee of total correction of bending
Recurrence of the curvature at a later stage
Significant bleeding or infection requiring further treatment
Nerve injury with temporary or permanent numbness of penis (more likely after Lue procedure) Impotence or difficulty maintaining erections (in up to 20% after Lue procedure and 7% after Nesbit’s procedure)
POSTOPERATIVE CARE
Depending upon the nature and length of the procedure and degree of postoperative pain, overnight observation is usually recommended.
Dressing — following the reconstructive procedure, a soft petroleum gauze is placed on the incision and covered loosely with a gauze pad. A light crepe bandage is placed around the penis to prevent swelling and care is taken not to make it too constrictive.
Pain management — Intravenous or oral pain medications are given, as needed.
The dressing and the catheter are removed the next morning and the wound checked. If all is well the patient is discharged home.
Patient instructions — Patients are instructed to:
- Resume activities as tolerated. Heavy lifting is avoided for four weeks.
- Return to work in a few days depending upon speed of recovery.
- Watch for signs of infection (ie, fever, redness, excess swelling, discharge, increasing pain), particularly if a prosthesis has been placed.
Sexual activity — Patient is instructed not to engage in sexual intercourse or masturbation for a minimum of 6 weeks.
FOLLOW UP CARE — Follow up in the outpatient is in 2 weeks to check the wound. If all is well a PDE5 inhibitor (Viagra, Cialis, Levitra) is started to help promote erections.
COMPLICATIONS
The complications associated with correction of Peyronie’s disease deformities are dependent upon the technique used for reconstruction. General complications include surgical site infection, penile hematoma, penile narrowing or indentation, phimosis, sensory abnormalities and erectile dysfunction.
Erectile dysfunction, like sensory abnormalities, is more likely to occur in procedures that require dissection and mobilization of the neurovascular bundle
Erectile dysfunction Erectile dysfunction (ED) is reported to occur in up to 20 percent of patients postoperatively. In retrospective reviews, placation techniques (ie, Lue procedure) have been reported to be associated with the least risk of erectile dysfunction compared with grafting procedures [8,11,16]. Patients with pre-operative ED are more likely to experience worsened sexual function, though ED can develop de novo. Up to 45 percent of patients with preexisting ED will suffer a further decline [20,21]. Long term, additional deterioration in both erectile and orgasmic function has been observed [20].
Graft complications The use of grafting materials is associated with additional complications that include: persistent pain which may be due to neurological injury, graft bulging (ie, herniation), graft infection, or graft contracture leading to penile shortening or recurrent curvature [14,22]. Surgical site infection can also occur at the site of autogenous tissue harvest.
OUTCOMES
With an appropriately-chosen technique, reconstruction for Peyronie’s disease achieves satisfactory results in the majority of men [1,13,20,22]. Long-term satisfaction with return to sexual activity was high for both patient (86 percent) and partner (77 percent) in a retrospective evaluation of 61 patients [23]. Curvature is corrected in most patients; however, minor residual and recurrent curvature is reported for all the techniques described.
Plication (Yachia, Nesbit) achieves penile straightening in 67 to 100 percent of patients with a low risk for postoperative sexual dysfunction [1,9,11,24,25]. The primary concern for these patients is the degree of penile shortening. While some degree of penile shortening occurs in all patients, few have difficulty with penetration [8]. Residual curvature rates vary from 7 to 21 percent, and may be due to suture absorption, slippage, or breakage [11].
For patients who undergo grafting procedures, patient satisfaction and curvature correction rates are the highest (>90 percent) with autogenous vein grafting [1,14,20,22,23,26,27]. Recurrent curvature occurs in 12 to 16 percent of patients following vein graft procedures [20,23].
The use of penile implants in the treatment of Peyronie’s disease produces satisfactory correction of curvature with adequate erectile function in greater than 85 percent of patients in most large series [1,17,28].
REFERENCES
1. Kadioglu A, Akman T, Sanli O, et al. Surgical treatment of Peyronie’s disease: a critical analysis. Eur
Urol 2006; 50:235.
2. Dean RC, Lue TF. Peyronie’s disease: advancements in recent surgical techniques. Curr Opin Urol 2004;
14:339.
3. Kalsi J, Minhas S, Christopher N, Ralph D. The results of plaque incision and venous grafting (Lue
procedure) to correct the penile deformity of Peyronie’s disease. BJU Int. 2005;95:1029-33
4. Levine LA, Lenting EL. A surgical algorithm for the treatment of Peyronie’s disease. J Urol 1997;
158:2149.
5. Kadioglu A, Tefekli A, Erol B, et al. A retrospective review of 307 men with Peyronie’s disease. J Urol
2002; 168:1075.
6. Greenfield JM, Lucas S, Levine LA. Factors affecting the loss of length associated with tunica albuginea
plication for correction of penile curvature. J Urol 2006; 175:238.
7. Brant WO, Bella AJ, Garcia MM, et al. Surgical Atlas. Correction of Peyronie’s disease: plaque incision
and grafting. BJU Int 2006; 97:1353.
8. Ralph DJ, al-Akraa M, Pryor JP. The Nesbit operation for Peyronie’s disease: 16-year experience. J Urol
1995; 154:1362.
9. Yachia D. Modified corporoplasty for the treatment of penile curvature. J Urol 1990; 143:80.
10. Brant WO, Bella AJ, Lue TF. 16-Dot procedure for penile curvature. J Sex Med 2007; 4:277.
11. Gholami SS, Lue TF. Correction of penile curvature using the 16-dot plication technique: a review of 132
patients. J Urol 2002; 167:2066.
12. Ralph DJ. The surgical treatment of Peyronie’s disease. Eur Urol 2006; 50:196.
13. Kendirci M, Hellstrom WJ. Critical analysis of surgery for Peyronie’s disease. Curr Opin Urol 2004;
14:381.
14. Breyer BN, Brant WO, Garcia MM, et al. Complications of porcine small intestine submucosa graft for
Peyronie’s disease. J Urol 2007; 177:589.
15. Knoll LD. Use of porcine small intestinal submucosal graft in the surgical management of Peyronie’s
disease. Urology 2001; 57:753.
16. Kalsi J, Christopher N, Ralph DJ, Minhas S. Plaque incision and fascia lata grafting in the surgical
management of Peyronie’s disease. BJU Int. 2006;98:110-115
17. Montorsi F, Guazzoni G, Bergamaschi F, Rigatti P. Patient-partner satisfaction with semirigid penile
prostheses for Peyronie’s disease: a 5-year followup study. J Urol 1993; 150:1819.
18. Wilson SK, Delk JR 2nd. A new treatment for Peyronie’s disease: modeling the penis over an inflatable
penile prosthesis. J Urol 1994; 152:1121.
19. Rahman NU, Carrion RE, Bochinski D, Lue TF. Combined penile plication surgery and insertion of
penile prosthesis for severe penile curvature and erectile dysfunction. J Urol 2004; 171:2346.
20. Montorsi, F, Salonia, S. Five year follow-up of plaque incision and vein grafting for Peyronie’s disease.
Eur Urol 2004; 3:33.
21. Montorsi F, Salonia A, Maga T, et al. Evidence based assessment of long-term results of plaque incision
and vein grafting for Peyronie’s disease. J Urol 2000; 163:1704.
22. El-Sakka AI, Rashwan HM, Lue TF. Venous patch graft for Peyronie’s disease. Part II: outcome analysis.
J Urol 1998; 160:2050.
23. Usta MF, Bivalacqua TJ, Sanabria J, et al. Patient and partner satisfaction and long-term results after
surgical treatment for Peyronie’s disease. Urology 2003; 62:105.
24. Gholami SS, Gonzalez-Cadavid NF, Lin CS, et al. Peyronie’s disease: a review. J Urol 2003; 169:1234.
25. Licht MR, Lewis RW. Modified Nesbit procedure for the treatment of Peyronie’s disease: a comparative
outcome analysis. J Urol 1997; 158:460.
26. Levine LA, Estrada CR. Human cadaveric pericardial graft for the surgical correction of Peyronie’s
disease. J Urol 2003; 170:2359.
27. Akkus E, Ozkara H, Alici B, et al. Incision and venous patch graft in the surgical treatment of penile
curvature in Peyronie’s disease. Eur Urol 2001; 40:531.
28. Wilson SK, Cleves MA, Delk JR 2nd. Long-term followup of treatment for Peyronie’s disease: modeling
the penis over an inflatable penile prosthesis. J Urol 2001; 165:825









